
Lecanemab is an IgG1 monoclonal antibody that binds and eliminates building blocks of amyloid plaques in the brain, thus helping to slow progression of Alzheimer disease.
Lacenemab: Discovery and Approval
Lecanemab (brand name Leqembi) was discovered by BioArctic, a Swedish biopharmaceutical company, in collaboration with Eisai Co., Ltd.
Since 2005 the team of Swedish biotech company BioArctic has been looking for a potential “cleaner of beta-amyloid protein deposits” in the brain. Previous studies have shown that beta-amyloid protein, which scientists believe to be “a brain junk“, plays a crucial role in the progression of Alzheimer’s disease.

At the start, lecanemab showed promising results in removing amyloid plaques in the brain. With phase II trials lecanemab showed main virtue of the sucessful meidication:
“the larger was a dose of the lecanemab; the better was the effect in removing amyloid debris”
The pivotal Phase III trial, known as Clarity AD cemented potential status as first Alzheimer’s breakthrough with 27% slowdown of disease progression comparing with placebo after 18 month of treatment.
Key Approval Timeline:
- July 2022: FDA granted Priority Review
- January 6, 2023: Received accelerated approval from the FDA
- July 6, 2023: Gained traditional FDA approval based on Phase III results
The FDA’s traditional approval represented a significant milestone as one of the first disease-modifying treatments for Alzheimer’s disease. Regulatory agencies in Japan and China approved lecanemab in September and December 2023, respectively.
The European Medicines Agency (EMA) followed with approval in early 2024, expanding global access to this novel treatment approach for early Alzheimer’s disease.
Lecanemab in Alzheimer Disease
Lecanemab represents a significant advancement in Alzheimer’s disease treatment through its targeted approach to amyloid beta aggregation. Recent clinical trials have demonstrated its efficacy in slowing cognitive decline in early-stage Alzheimer’s disease patients.
What is Alzheimer?
Alzheimer’s disease (AD) also known as Alzheimer dementia accounts for 80% of all cases of memory loss. It affects approximately 6.5 million Americans and is projected to nearly triple by 2060 as the population ages. There are three main features of AD:
- The decline of cognitive abolities is serious enough to interfere with daily activities
- AD is progressive disorder, so it worsens over time
- There is no cure for the Alzheimer’s dementia and till the recent years there was no reliable medication to slow the progression of this dibilitating disease
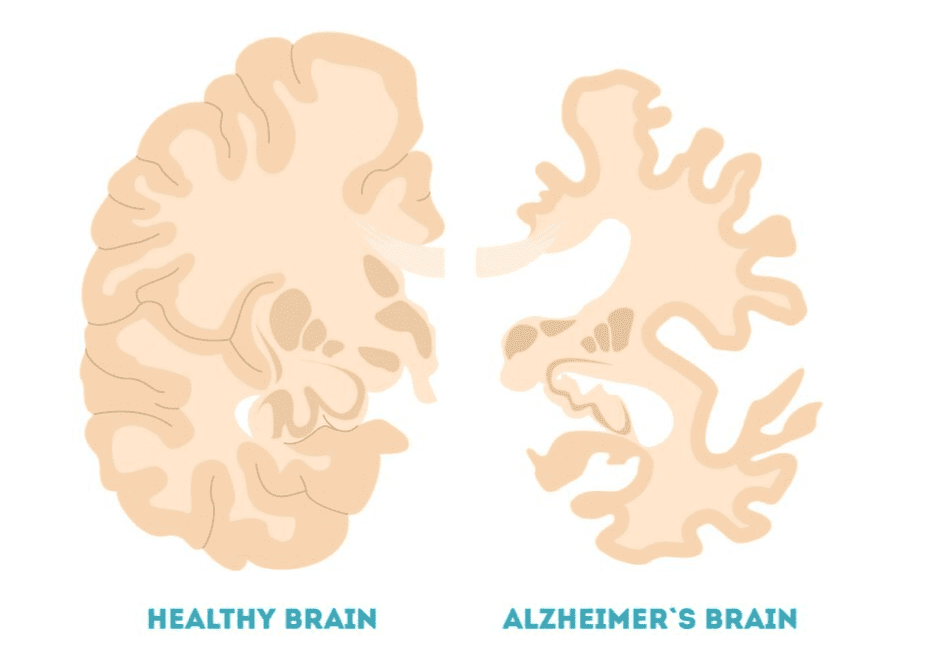
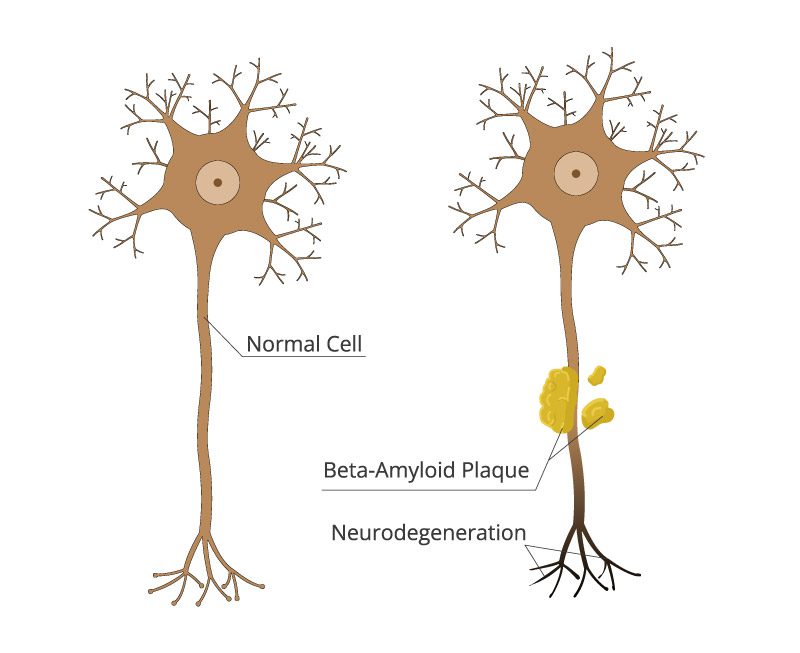
Changes in Alzheimer’s Brain
Now let’s take a microscope and look at the AD’s brain tissues. There are two main “hystological landmarks” that you don’t usually see in normal brains:
- amyloid beta plaques, discovered by no other than Dr. Alois Alzheimer
- tau neurofibrillary tangles, not as speciifc, as the amyloid debris, as tangles are found in other neurological disorders called taupaties, but stiil a significant biomarker of AD.
Apart of playing a role of “biomarkers”, which help to diagnose the disease, these protein aggregates have a significant role in development and progression of AD.
Role of Amyloid Beta
Amyloid beta (Aβ) is a soluble protein found in healthy brain cells. Although scientists are still puzzling out what it is, evidence suggests it might help neurons to grow and survive. Some researchers believe it has anti-cancer activities and helps glia cells (neural babysitters) to repulse infections and pathogens.
As in many molecules, Aβ has different forms: some of them good and some of them not. A low level of Aβ-42 in blood and CFS, and a high level of Aβ-40 is certainly toxic for our brain and are associated with cognitive decline. The test measuring their ratio in the blood is approved in the USA as an early biomarker of Alzheimer’s disease.
Toxic Aβ residues bind each other forming a toxic soluble component called oligomer. Many labs developed a test to measure the level of the Aβ Oligomer as an early marker of AD.
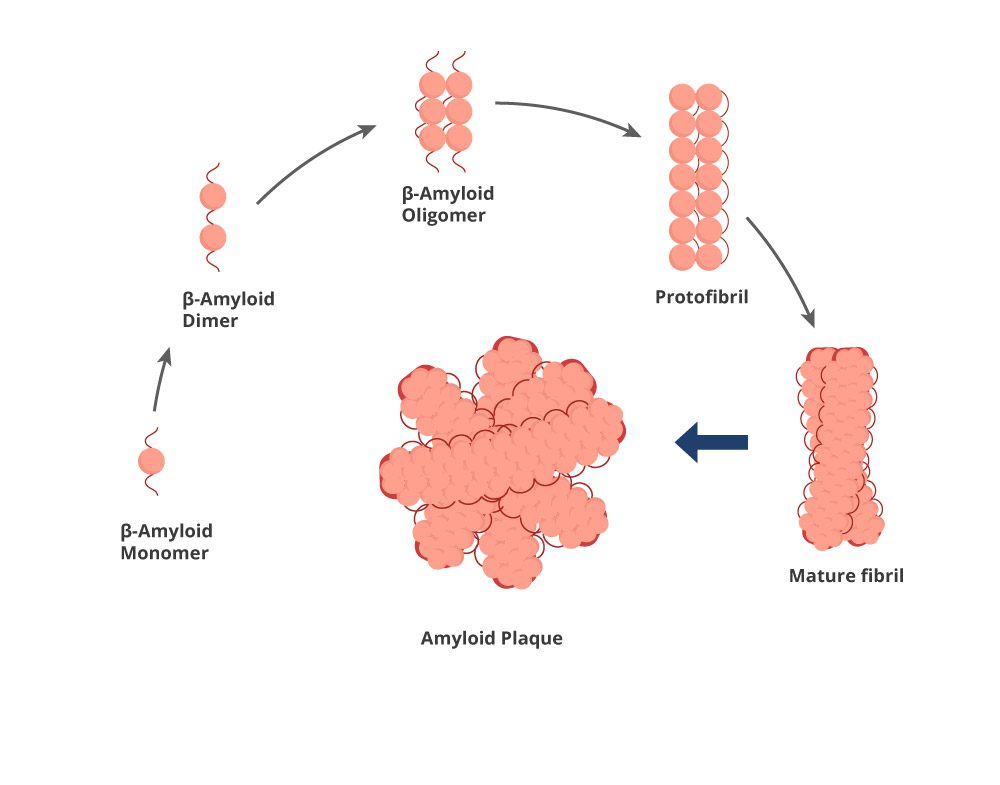
Amyloid oligomers continue to aggegragate forming protofibril – main target of lecanemab, which is also an intermidiary product in so called “Amyloid aggregation pathway”. Still soluble, several protofibrils form a mature fibril, which precipitates and forms a an amyloid debris.
Life of neural cells gets significantly distrupted by amyloid junk:
- It slows down neural impulses
- It attract attention of the immune system, that promotes inflammation of the neurons
- It disrupts neaural recovery and stresses out neural cells
Previous Attempts to Target Amyloid
Solanezumab is a humanized monoclonal IgG1 antibody directed against amino acids13–28 of amyloid. It recognizes soluble monomeric Aβ and does not recognize amyloid plaques. The drug has been tested both in sporadic and familial AD patients and failed to show any clinical improvement.
Crenezumab binds oligomeric and fibrillar Aβ with high affinity, promising
Gantenerumab is a fully human IgG1 antibody that binds Aβ fibrils. It has two epitopes on Aβ: one in the N-terminal region (amino acids 3–11) and another in the central region (amino acids 18–27). Clinical trials showed it is 8% more effective than placebo, which is disappointing.
Second-generation antibodies like aducanumab showed more promise. However, conflicting trial results and concerns about amyloid-related imaging abnormalities (ARIA) complicated its regulatory path.
Several gamma-secretase inhibitors also failed in trials due to off-target effects and safety concerns. Beta-secretase inhibitors similarly disappointed, highlighting the complexity of targeting the amyloid pathway effectively.
Lecanemab in Action
Amyloid-beta Targeting
Lecanemab is an IgG1 monoclonal antibody that selectively binds to soluble Aβ protofibrils. The precise binding site is still a secret, but studies hint it lies between amino acids 1 and 15 of Aβ.
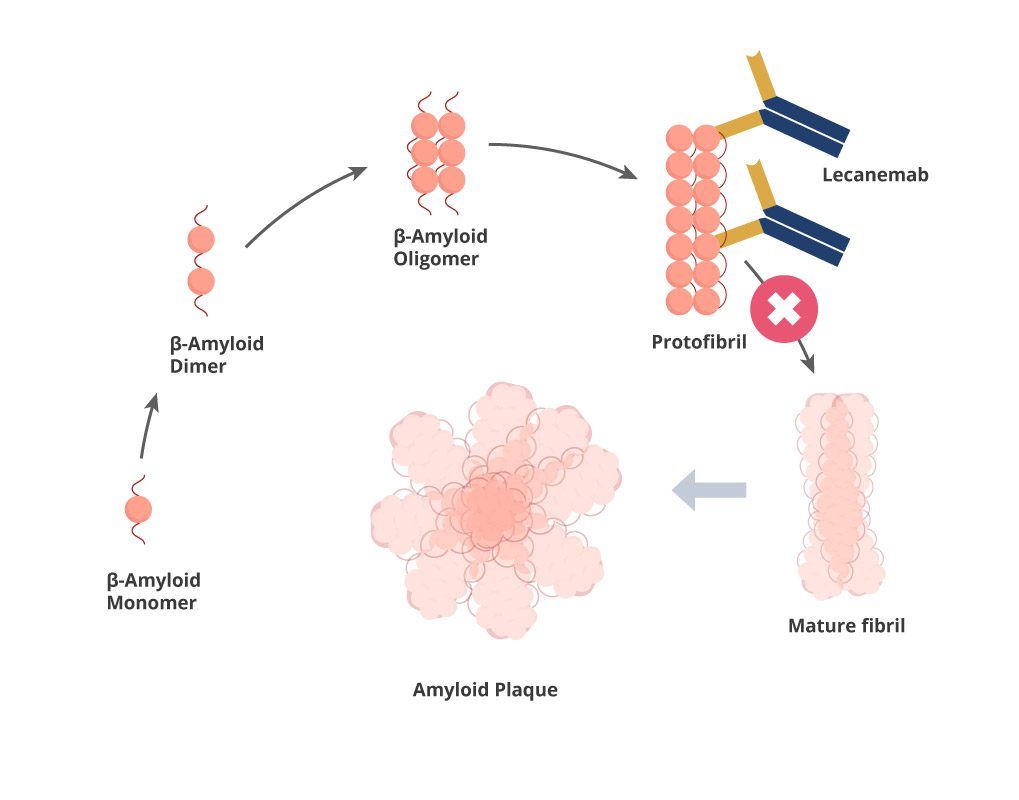
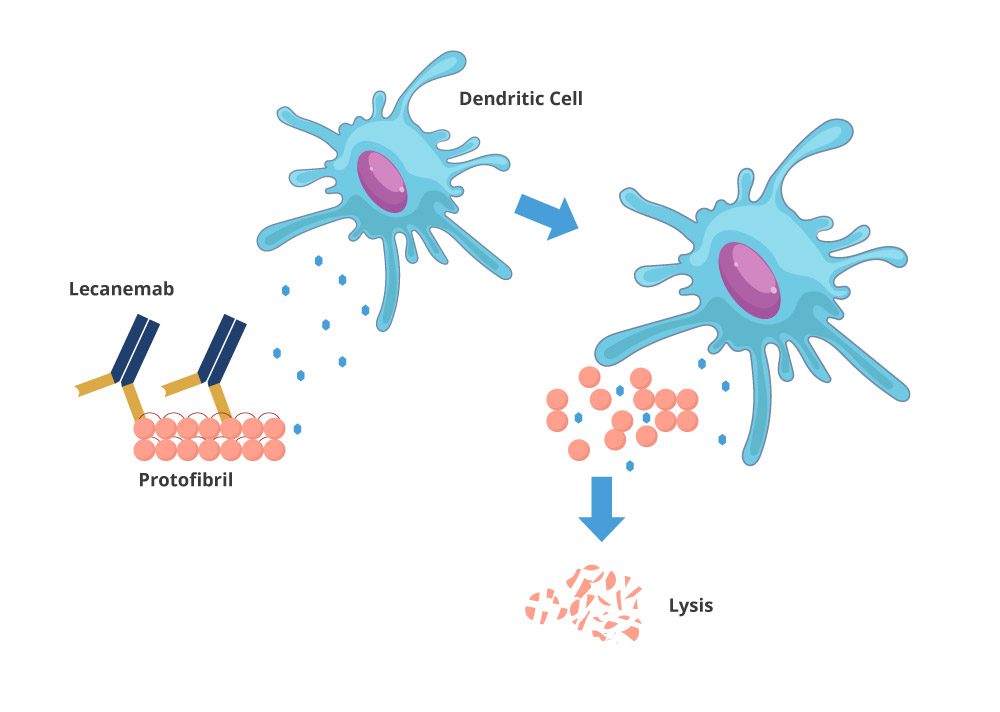
The antibody binds with high affinity to amyloid-beta protofibrils, creating immune complexes that can be cleared through various elimination pathways:
- Microglia cells, which combine functions of bodyguard and babysitter for neurons, would devour fibrills marked by the Lecamab
- Direct neutralization of toxic protofibrils by antibodies
How effective is lecanemab for Alzheimer’s disease
Clinical trials have demonstrated significant efficacy for lecanemab in early Alzheimer’s disease. The phase 3 CLARITY-AD trial showed a 27% slowing of cognitive decline compared to placebo over 18 months, as measured by the Clinical Dementia Rating Scale.
Biomarker studies confirm lecanemab substantially reduces amyloid plaques 65-80% as shown during pet imaging of patients receiving lecanemab.
The drug demonstrates greater efficacy when administered on early stages of the disease, particularly in patients with mild cognitive impairment or early signs of AD. Treatment benefits appear dose-dependent.
Despite measurable benefits, lecanemab does not halt disease progression completely. Treatment effects are relatively modest in terms of slowing rates of cognitive decline, resulting in 4-6 month delay in symptom progression.
How Would you Take Lecanemab
The doctors administer lecanemab via I.V. route. Medical supervision is must, as studies showed 28% of patients receiving lecanemab compalined post-injection complications.
Before you take lecanemab
Patients should undergo comprehensive medical evaluation before starting lecanemab treatment. This includes brain MRI scans to assess for amyloid-related imaging abnormalities (ARIA) and to establish a baseline for monitoring.
Genetic testing for APOE ε4 allele status may be recommended, as carriers have a higher risk of developing ARIA. Healthcare providers should review the patient’s complete medication list to identify potential interactions.
Patients with a history of cerebral hemorrhage, unstable cardiovascular disease, or certain autoimmune conditions may not be suitable candidates. A thorough discussion about potential benefits and risks should take place before initiating treatment.
Medical professionals must ensure patients understand the commitment to regular infusions and monitoring appointments. Patients should report any new neurological symptoms immediately during treatment.
Does Lecanemab interact with other medications
Lecanemab may interact with anticoagulant and antiplatelet medications, potentially increasing the risk of cerebral hemorrhage. Patients taking warfarin, direct oral anticoagulants, or antiplatelet drugs require careful monitoring.
Combinations of monoclonal antibodies targeting amyloid has not been studied and is not recommended. Potential interactions with cholinesterase inhibitors and memantine (common Alzheimer’s medications) appear minimal based on available data.
Medications that affect the immune system might theoretically impact lecanemab’s efficacy, though clinical evidence is limited.
Is it Safe to Take Lecanemab?
Safety concerns with lecanemab primarily revolve around amyloid-related imaging abnormalities (ARIA) and practical monitoring requirements for patients undergoing treatment.
Previous trials show
The pivotal Phase 3 CLARITY-AD trial provided crucial safety data for lecanemab. Among 898 participants receiving the drug, approximately 21.3% developed ARIA-E (edema) compared to 9.3% in the placebo group. Most ARIA-E cases were asymptomatic, detected only through routine MRI monitoring.
ARIA-H (hemorrhage) occurred in 17.3% of lecanemab-treated participants versus 9.0% in the placebo group. The trial reported 0.7% mortality in both treatment and placebo arms, suggesting no significant increase in death rate.
Safety monitoring included regular MRIs during the first 14 weeks of treatment. APOE ε4 carriers showed higher ARIA risk, with 30.8% of homozygotes developing ARIA-E compared to 13.2% in non-carriers.
Potential side effects
Infusion-related reactions represent another significant concern, affecting 26.4% of lecanemab recipients compared to 7.4% in the placebo group. These reactions typically manifest as flu-like symptoms, headache, or nausea during or shortly after administration.
Most infusion reactions occur during early treatments and diminish with subsequent doses. Premedication with antihistamines, antipyretics, or corticosteroids may help manage these reactions.
Other reported side effects include headache (17%), falls (17%), and diarrhea (9%). Serious adverse events occurred in 14% of lecanemab-treated participants versus 11% in the placebo group.
Long-term safety data remains limited as the longest clinical trials lasted 18 months. Ongoing monitoring through registry studies and post-approval surveillance will provide critical information about rare side effects and long-term safety profiles.
Other promissing drugs to treat Alzheimer
While Lecanemab offers a promising approach to treating Alzheimer’s disease, several other therapeutic candidates are in various stages of development. These emerging treatments target different pathological mechanisms and aim to either slow disease progression or alleviate symptoms through novel pathways.
Potential Therapeutic targets for Alzheimer disease
Tau protein aggregation represents a significant therapeutic target beyond amyloid. Anti-tau antibodies like Zagotenemab and Semorinemab aim to prevent tau tangles formation and spread. Though recent trials have shown mixed results, ongoing research continues to refine these approaches.
Neuroinflammation modulation offers another promising avenue. Drugs targeting microglial activation, such as GC021109 and masitinib, show potential by dampening inflammatory responses in the brain that contribute to neurodegeneration.
Metabolic dysfunction correction through drugs like T3D-959, which targets PPAR delta/gamma pathways, addresses glucose metabolism abnormalities common in Alzheimer’s patients. This approach recognizes the “type 3 diabetes” hypothesis of Alzheimer’s disease.
Neuroprotective strategies utilizing compounds like Blarcamesine (ANAVEX2-73) aim to activate sigma-1 receptors, potentially reducing oxidative stress and improving cellular resilience. Early clinical trials have shown promising cognitive benefits.
Current Alzheimer pipeline
Donanemab, developed by Eli Lilly, has shown promising results in Phase 3 trials with significant plaque reduction and slowed cognitive decline. It received Breakthrough Therapy designation from the FDA in 2021.
Gantenerumab, while failing to meet primary endpoints in pivotal trials, continues development with modified dosing strategies. Swiss pharma giant Roche remains committed to exploring its potential benefits.
ACI-35 represents a novel vaccine approach targeting pathological tau. This immunotherapy stimulates antibody production against phosphorylated tau without triggering harmful autoimmune responses.
Small molecule approaches include SAGE-718, an NMDA receptor modulator showing improvements in executive function in early trials. PQ912, a glutaminyl cyclase inhibitor, aims to reduce production of pyroglutamate-modified Aβ, a particularly toxic form.
Non-pharmaceutical treatment of Alzheimer disease
Cognitive stimulation therapy (CST) provides structured activities designed to enhance cognitive function and social interaction. Multiple studies demonstrate moderate improvements in cognition and quality of life when delivered in group settings.
Physical exercise programs show remarkable benefits with aerobic activities like walking potentially slowing cognitive decline. Research indicates 150 minutes of moderate exercise weekly may help maintain cognitive function.
Dietary interventions, particularly the MIND diet (Mediterranean-DASH Intervention for Neurodegenerative Delay), have shown promising results. This approach emphasizes leafy greens, berries, nuts, and limits red meat and processed foods.
Multimodal approaches combining lifestyle interventions yield synergistic benefits. The FINGER study demonstrated that simultaneous nutritional guidance, exercise, cognitive training, and vascular risk monitoring significantly reduced cognitive decline compared to single interventions.
Summary
Lecanemab is a monoclonal antibody designed to target and remove amyloid beta (Aβ) plaques in Alzheimer’s disease. It specifically binds to soluble Aβ protofibrils, which are considered more neurotoxic than other forms of amyloid aggregates.
The drug works through immunotherapy principles by recognizing the N-terminus of Aβ protofibrils with high selectivity. This binding gives a signal to glia to clear amyloid plaques.
Clinical trials have demonstrated lecanemab’s effectiveness in reducing amyloid plaque burden by approximately 27% compared to placebo groups. PET imaging studies confirm significant reductions in brain amyloid levels following treatment.
The mechanism involves three key steps:
- selective binding to protofibrils,
- recruitment of microglia,
- clearance of Aβ aggregates.
This targeted approach minimizes interactions with monomeric Aβ, which may have physiological functions in the brain.
Lecanemab’s specificity distinguishes it from earlier anti-amyloid antibodies. By focusing on protofibrils rather than all amyloid forms, it satnds out as a safer and more specific option.
The drug’s concentration in brain circulation is 500 time less of its level in peripheral blood. Although it might seem to be poor result for any small molecule, lecanemab crosses blood brain barrier much better than other representatives of the class.